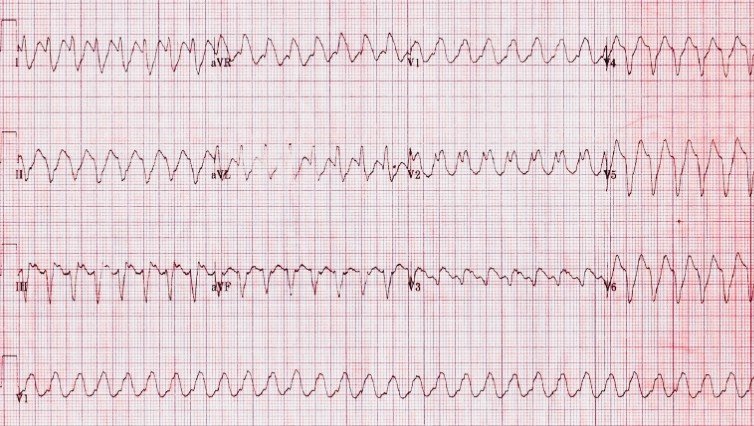
A 2-month-old infant is 8 hours post–VSD patch closure and PDA ligation. Temperature is 38.3°C, lactate is rising, and CVP is elevated. Temporary atrial and ventricular epicardial pacing wires are in place. The surface ECG (Lead II) and atrial electrogram (AEG) from pacing wires are shown above.
Quiz Question
What is the most likely rhythm diagnosis, and what is the immediate management priority?
Diagnosis: Postoperative Junctional Ectopic Tachycardia (JET)
ECG & AEG Interpretation
Surface ECG (Lead II):
⦁ Narrow QRS tachycardia
⦁ Regular ventricular rate ~190–210/min
⦁ P waves difficult to discern or dissociated
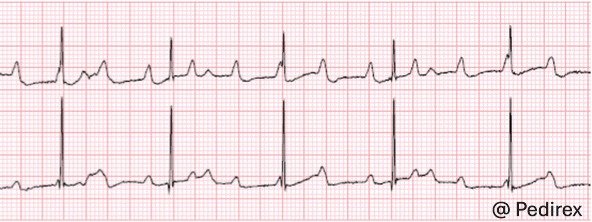
Atrial Electrogram (AEG):
⦁ Ventricular electrograms preceding atrial signals
⦁ AV dissociation
⦁ Ventricular rate faster than atrial rate
This confirms a junctional focus driving the rhythm, not sinus tachycardia or reentrant SVT.
Why This Is Dangerous in Infants
⦁ Loss of AV synchrony → ↓ ventricular filling
⦁ Particularly poorly tolerated in:
⦁ Small ventricles
⦁ Post-CPB myocardial edema
⦁ RV dysfunction
⦁ Can precipitate:
⦁ Low cardiac output syndrome
⦁ Escalating inotrope requirement
⦁ Cardiac arrest if untreated
JET is common after:
⦁ VSD repair
⦁ Tetralogy of Fallot repair
⦁ AV canal repair
Management Strategy (PICU-Level)
Immediate Priorities:
⦁ Reduce myocardial irritability
⦁ Treat fever aggressively
⦁ Optimize sedation/analgesia
⦁ Correct electrolytes (Mg >2, K high-normal)
⦁ Reduce catecholamine exposure
⦁ Wean inotropes if possible
⦁ Controlled cooling
⦁ Target 35–36°C if persistent
⦁ Antiarrhythmic therapy
⦁ Amiodarone infusion (first-line in many centers)
⦁ Procainamide alternative in selected cases
⦁ Restore AV synchrony
⦁ Atrial overdrive pacing if atrial rate can exceed JET rate
⦁ AV sequential pacing to improve cardiac output
Refractory cases:
⦁ Deep sedation ± paralysis
⦁ Consider ECMO if profound LCOS
Pearls
⦁ Adenosine does not terminate JET.
⦁ The diagnostic clue is ventricular rate faster than atrial rate on AEG.
⦁ JET is an automatic tachycardia, cardioversion is ineffective.
⦁ Temperature control is therapeutic, not just supportive.